



Meniscus injuries
Concerning ruptures of the meniscus one can distinguish acute injuries (most of the time these are sport injuries at football, handball, basketball or skiing or when twisting the knee while standing up from the squat) from degenerative meaning due to wear damages. Injuries oft he medial meniscus are way more frequent than ones of the lateral, as the medial meniscus is grown tightly together with the collateral ligament.

There are different forms of tears (like cloth tears, radial tears, bucket handle tears, horizontal tears etc.)
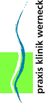
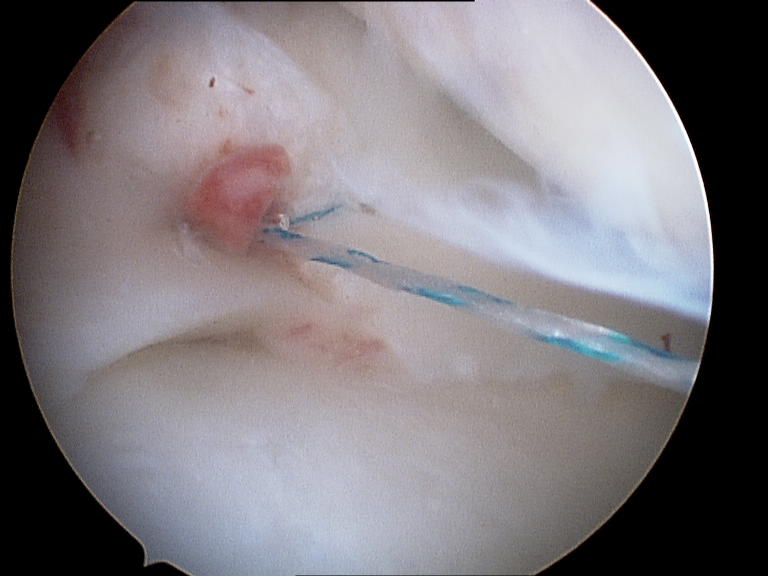
before the meniscal suture
After a thorough bodily examination the torn meniscus can be diagnosed in conjunction with x-rays, sonography and probably MRT. Occasionally, only the arthroscopy reveals a tear not found during the examinations before, because only the movement of the knee under arthroscopic control makes the tear visible.
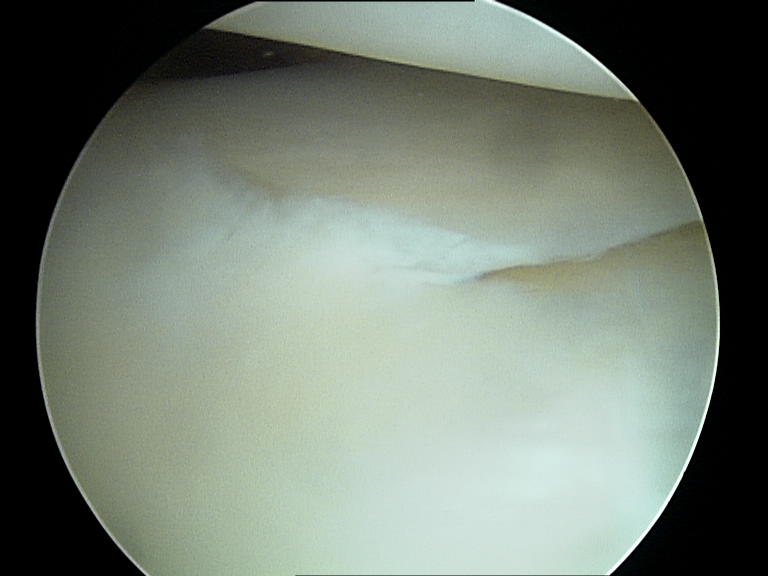
under the MRT before...

In case of a diagnosed meniscus damage one would tend early to a surgery (knee joint arthroscopy = knee endoscopy), even if no or only mild pains exist, as due to the defective meniscus a constant friction of untypical pressure peaks against the cartilage takes place, which can rapidly lead to cartilage damages. Most of the time this stimulus does not stop, as the meniscus is supplied with blood only near its base and hardly heals by itself.
A good healing tendency exists only in the red zone. The blood circulation and thus the healing tendency decreases inwardly and constantly until zone III. The constant Reibebewegungen of the defective meniscus in case of no treatment lead to recurring pains under load. pinching effects, knee joint swellings and secondary damages at the cartilage surfaces and thus to an premature arthrosis.
Occasionally, cysts form at the base of the meniscus, a so-called ganglion (or meniscus ganglion) develops. A ganglion is filled with a mostly gel-like liquid. In most cases a torn meniscus exists at the same time, which should definitely be treated. The removal of the ganglion without a correcting of the cause makes no sense at all.
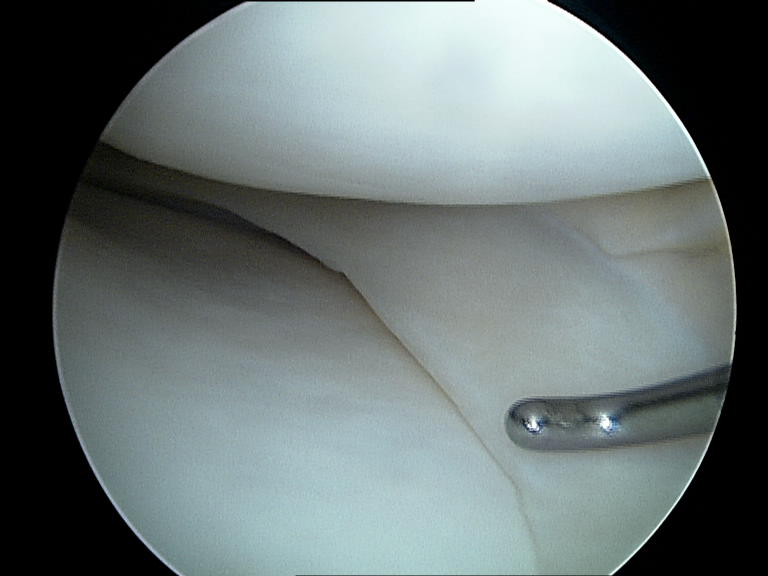
During the knee joint arthroscopy only the torn part of the meniscus is removed and the meniscus is smoothed carefully. One can try to preserve the meniscus in order to minimize the risk of arthrosis, which exists after the partial removal of the meniscus.
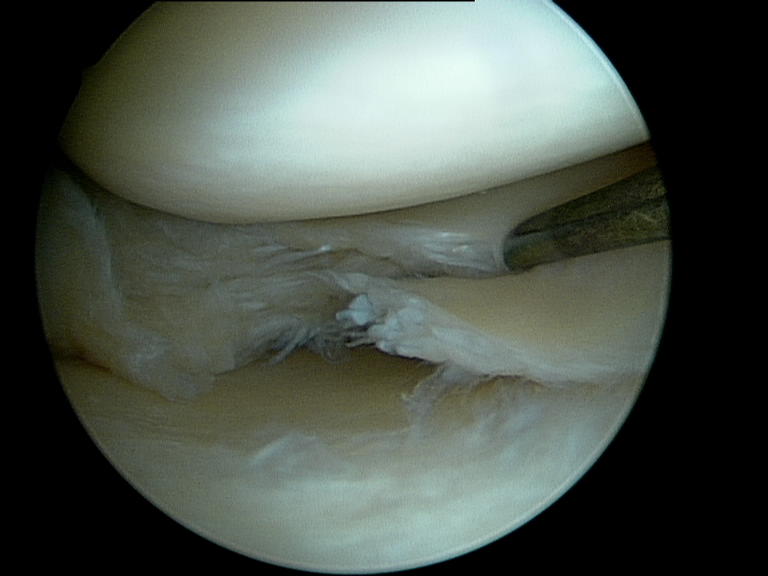
The meniscus is sutured especially in case of tears in the RR-zone.
The advantage of the meniscus suture is, that the slightly increased danger for an arthrosis, which also exists after the partial removal oft he meniscus, can be minimized.
The disadvantage is, that the rehabilitation especially in sports takes much longer and that with a probability of up to 25% a relatively high danger for a new tear exists. Optimum healing terms are only given, if the meniscus refixation could had been performed in the RR-zone and if the tear was fresh.
Rehabilitation
After a meniscus surgery (partial removal of the defective meniscus) the strain on the leg is relatively fast possible, as long as the pains allow it. Walking supports are mostly only needed for a few days. After two weeks riding a bicycle or ergometer training is allowed, after four weeks running sports, after 6 weeks ball sports or skiing.
After a meniscus suture or meniscus refixation the load takes place after 1-2 weeks in an orthosis (knee splint) with a temporary (6-8 weeks) limited mobility. Deep squads and sporty load should remain undone for 12 weeks.
Meniscus replacement
If a meniscus suture is not possible and if more than a quarter of the meniscus has to be removed, a replacement with a collagen meniscus implant (CMI) can make sense, especially for young people and children.

Many studies have confirmed the effectiveness of these implants as a replacement for the medial and lateral meniscus (www.ivysportsmed.com). For the functioning of the CMI an intact and stable border of the remaining meniscus is necessary. If this one is missing as well, then only a meniscus transplantation with a fitting corpse transplant (Allograft) can still be performed. Due to its low availability and the high legal requirements this procedure is a rarity in Germany.







 und Außenmeniskus (unten)")